BUNIA, Democratic Republic of the Congo — A growing Ebola outbreak caused by the rare Bundibugyo strain in eastern Democratic Republic of the Congo (DRC) and neighboring Uganda carries high transmission risks at national and regional levels, while the global threat remains low, the World Health Organization confirmed Wednesday.
The updated risk assessment comes as response teams race to contain an outbreak that has already claimed 134 suspected lives, and WHO’s DRC mission lead warned the epidemic could persist for at least two more months even as aid operations scale up.
The WHO previously designated the outbreak a Public Health Emergency of International Concern (PHEIC), a status that demands a coordinated, global collective response to curb spread. On Tuesday, the agency already raised alarm over the outbreak’s alarming growth trajectory and rapid transmission pace.
Health experts and frontline aid workers note the outbreak has been marked by critical early setbacks: the rare Bundibugyo strain spread undetected for weeks after the first recorded fatality, as authorities initially tested for more common Ebola variants and returned negative results. Currently, no officially approved treatments or licensed vaccines exist specifically for the Bundibugyo strain, leaving response teams with limited targeted tools. Local residents already grappling with long-running instability report sharp price hikes for basic protective supplies, including face masks and disinfectants, as demand surges.
As of Wednesday, WHO Director-General Tedros Adhanom Ghebreyesus confirmed 51 confirmed cases across DRC’s conflict-affected Ituri and North Kivu provinces, plus two additional confirmed cases in Uganda. There are also nearly 600 additional suspected cases and deaths, and Tedros warned case counts will continue to climb in the coming weeks. “We know that the scale of the epidemic is much larger,” he stated, adding that upward revisions to case numbers are expected as surveillance expands.
Multiple structural challenges continue to hamper containment efforts. The first recorded death from the current outbreak was recorded in Bunia on April 24, but official confirmation of the strain took weeks. The victim’s body was repatriated to Mongbwalu, a populous gold-mining region that has since become the outbreak’s epicenter, a delay that DRC Health Minister Samuel Roger Kamba confirmed directly fueled the epidemic’s escalation. To date, response teams have not yet identified the index case (patient zero) of the outbreak, WHO’s DRC lead Dr. Anne Ancia confirmed.
Beyond detection delays, large cross-border population movements in the region and a long-running pre-existing humanitarian crisis have complicated response work. Large swathes of eastern DRC remain controlled by armed rebel groups, blocking aid teams from accessing high-risk areas. Dr. Ancia added that recent funding cuts have also severely undermined the work of frontline humanitarian organizations, stretching already thin resources even thinner.
To address the lack of targeted vaccines, DRC’s national biomedical research institute expects imminent shipments of an experimental broad-spectrum Ebola vaccine developed by Oxford University researchers from the United States and the United Kingdom. “We will administer the vaccine and see who develops the disease,” explained Jean-Jacques Muyembe, leading virus expert at the institute, outlining the trial protocol for the unapproved product.
The United States has also committed additional support: U.S. Secretary of State Marco Rubio announced Tuesday that the Trump administration will prioritize funding for 50 new emergency clinics in affected regions, building on the $13 million Washington has already allocated to the response, with more funding to come.
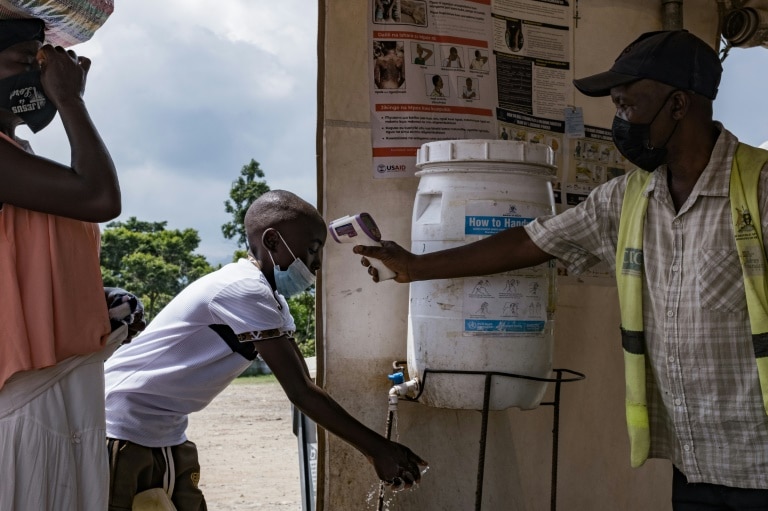
On the ground in Bunia, where the first fatality was recorded, daily life has partially continued: schools and churches remained open Wednesday, though many residents now wear face masks in public. Still, supply shortages have sent prices skyrocketing: local residents report that a bottle of disinfectant that previously cost 2,500 Congolese francs now retails for as much as 10,000 francs ($4.4), and masks have become nearly impossible to source at any price. “It’s truly sad and painful because we’ve already been through a security crisis, and now Ebola is here too,” said Bunia resident Justin Ndasi. “We have to protect ourselves to avoid this epidemic.”
Frontline medical groups say local health infrastructure is already overwhelmed. Trish Newport, emergency program manager for Doctors Without Borders (MSF), said her team identified multiple suspected cases over the weekend at Bunia’s Salama Hospital, which lacks any dedicated Ebola isolation ward. When they tried to transfer patients to other facilities, every available bed was already occupied. “Every health facility they called said, ‘We’re full of suspects cases. We don’t have any space.’ This gives you a vision of how crazy it is right now,” Newport said.
In Mongbwalu, the outbreak’s epicenter, the border with Uganda remains open and commercial gold mining operations continue, according to local civil society leader Chérubin Kuku Ndilawa. While widespread panic has not taken hold, with residents continuing daily routines, community awareness efforts are just starting to scale up. Ndilawa added that a lack of basic public health infrastructure, including handwashing stations in high-traffic public areas, continues to hinder containment work. At Mongbwalu General Hospital, former director Dr. Didier Pay reported the facility is currently caring for around 30 confirmed Ebola patients, and a local medical technology student died from the virus Wednesday morning.
AP writers Jamey Keaten in Geneva and Wilson McMakin in Dakar contributed reporting to this article. AP’s global health and development coverage in Africa is supported by funding from the Gates Foundation; the AP maintains full editorial control over all content.