A high-stakes diplomatic gathering intended to strengthen ties between India and the entire African continent has been called off at the eleventh hour, derailed by the spreading Ebola outbreak currently impacting the Democratic Republic of Congo and Uganda. The fourth iteration of the India-Africa Forum Summit, which was slated to take place in New Delhi between May 28 and 31 after more than a decade since the last convening, will be rescheduled for a later date, according to a joint statement released Thursday by the Indian government and the African Union.
The joint announcement cited the rapidly worsening public health crisis unfolding across central Africa as the core reason for the delay, noting that a new confirmed date for the summit will be made public once the outbreak is under control. This decision comes just days after the World Health Organization (WHO) upgraded the current outbreak to the highest level of global alert: a Public Health Emergency of International Concern (PHEIC).
As of the latest WHO update, the outbreak has already recorded 600 suspected cases and 139 suspected deaths across affected regions. To date, all reported infections have been restricted to the African continent, but public health experts have warned that this outbreak presents unique and unprecedented challenges. Unlike previous Ebola events, the current outbreak is driven by a rare strain of the virus for which no licensed vaccine currently exists, and the epicenter of the spread is located in a conflict-impacted region, complicating rapid response and containment efforts.
Ebola is a severe, often fatal viral illness that originates in animal populations, most commonly fruit bats. Spillover into human populations typically occurs when humans handle or consume infected wild animals. After an incubation period ranging from two to 21 days, symptoms emerge abruptly, beginning with flu-like indicators including fever, headache, and fatigue. As the virus progresses, patients develop severe vomiting and diarrhea, often progressing to organ failure. A subset of patients also experience internal and external bleeding. The virus spreads between humans through direct contact with infected bodily fluids, such as blood or vomit.
Historically, Ebola outbreaks were small and easily contained to remote, sparsely populated rural areas. But experts note that accelerating urbanization has pushed growing human populations closer to the natural reservoirs of the Ebola virus, steadily increasing the risk of future spillover events and large-scale outbreaks.
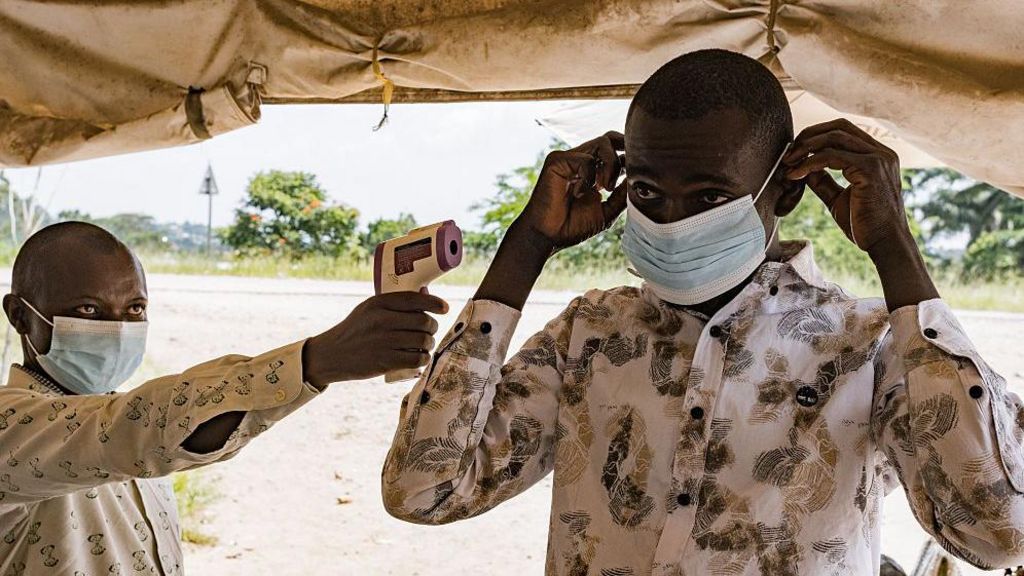
Even though no confirmed Ebola cases have been detected within India’s borders to date, national health authorities have moved quickly to implement preventive measures. On Thursday, India’s Directorate General of Health Services released an official public health advisory for all passengers arriving from or transiting through Ebola-affected nations. The advisory directs travelers to immediately contact airport health officials and seek urgent medical care if they develop any characteristic Ebola symptoms within 21 days of travel, or if they have had close direct contact with a confirmed or suspected infected person.