A rapidly expanding Ebola outbreak in the eastern region of the Democratic Republic of the Congo (DRC) has sparked widespread public fear, triggered an international public health emergency declaration, and left more than 130 people dead as response teams race to contain a virus that spread undetected for weeks.
As of Tuesday, official data counts 513 suspected cases across multiple provinces, with 136 confirmed fatalities in the DRC and one additional death recorded in neighboring Uganda. Cases have already spread beyond the Ituri province epicenter to reach major population centers including Butembo, Goma, and areas of South Kivu, raising alarm among public health authorities about the outbreak’s trajectory.
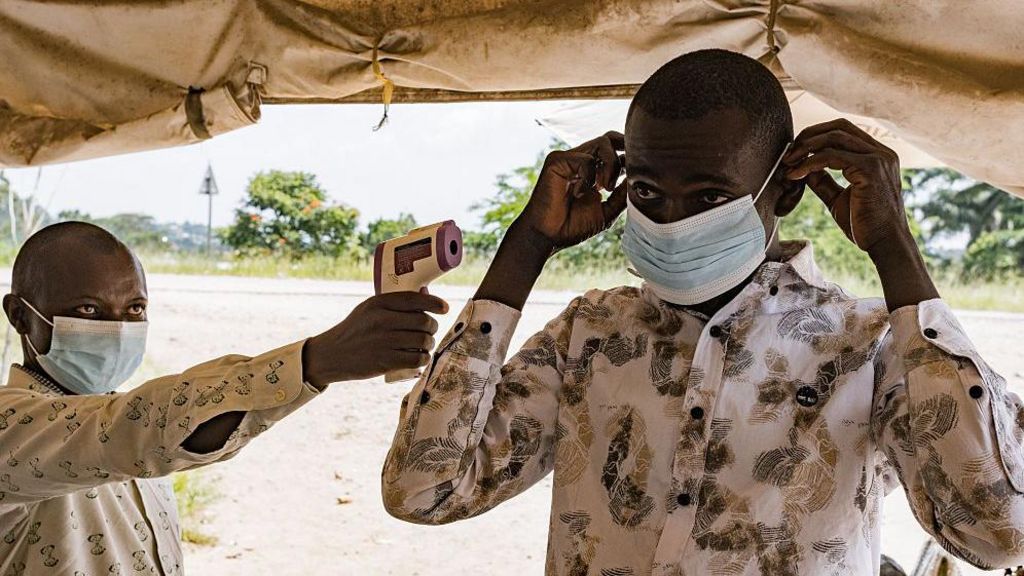
Local communities in the gold-mining hubs at the center of the outbreak have been gripped by anxiety since the first cases emerged. “Ebola has tortured us,” a 20-something taxi driver in Rwampara told reporters. “I am scared because people are dying very fast… We are really afraid.” Local resident Fred Kiza added that widespread fear is an unavoidable response to the crisis, noting that basic protective supplies like face masks remain scarce for at-risk communities.
Congolese Health Minister Dr Samuel Roger Kamba, who visited the Ituri outbreak epicenter over the weekend, acknowledged that response teams are already playing catch-up against a virus that may have begun circulating long before it was first formally detected on April 24. The presumed index patient, a nurse who died in the provincial capital of Bunia, was buried in Mongwalu, another gold-mining town that has recorded the majority of the outbreak’s suspected cases and deaths alongside neighboring Rwampara.
Official community reporting of unexplained deaths and illness only began on May 8, meaning many early fatalities went unrecorded and uninvestigated. “At community level, this hasn’t been effective,” Dr Kamba explained. “It means someone may have died before him [the presumed index case], or someone else may have been sick before him, but no one reported it. We really need to look within the community to understand what happened – how people became ill and sometimes even died without any report being filed.”
Complicating detection and response is the specific strain of Ebola causing this outbreak: the Bundibugyo variant, which is far less common in the DRC than the more widely known Zaïre strain. The DRC is currently facing its 17th Ebola outbreak, and local health systems were mostly prepared for the Zaïre variant. Before this current event, Bundibugyo had only caused two small outbreaks, in 2007 and 2012, and has a documented mortality rate of around 30 percent.
The Bundibugyo strain also presents more subtle symptoms than many people familiar with Ebola expect, leading to dangerous diagnostic delays. “There is heavy bleeding everywhere, very high fever. But Bundibugyo can show fewer obvious signs, which delays diagnosis because people think, ‘No, this is just malaria,’” Dr Kamba said. In some Mongwalu communities, early deaths were incorrectly attributed to witchcraft rather than a contagious virus, fueling a local belief called the “coffin phenomenon” that anyone who touches an infected person’s coffin will also die.
International aid group Save the Children confirmed that the Bundibugyo strain had never been detected in Ituri before this outbreak, and initial limited testing only screened for the Zaïre strain, returning false negative results. “By the time the Bundibugyo strain was detected, it had already spread quite far. We are in a game of catch-up,” said Greg Ramm, the organization’s DRC representative.
Five days after the outbreak was formally declared, none of the major affected urban centers—Bunia, Butembo, and Goma, each home to hundreds of thousands of residents—have a fully operational Ebola treatment center, leaving local residents frustrated with the slow pace of response. “If there’s no treatment centre here in the capital, then what about other areas?” one Bunia resident asked.
In Goma, eastern DRC’s largest city and a major regional trading hub, basic public health safety measures—including social distancing, limited gatherings, regular handwashing, and mask-wearing—are widely ignored. Many residents say daily survival takes priority over virus prevention rules, while low awareness contributes to low compliance. “It’s too much to ask people struggling to eat to follow these rules,” one local resident explained. Local journalist José Mutanava noted that he wears a mask for work, but barely any other residents in the city do.
The unstable security environment in eastern DRC adds another layer of complexity to response efforts. Four of the five affected administrative areas are in Ituri, while Goma in North Kivu is currently controlled by M23 rebel forces, and Butembo, North Kivu’s second-largest city, faces ongoing militia violence. Hundreds of thousands of people are already displaced in the region, and local healthcare systems were already severely stretched before the outbreak began.
“The Ebola outbreak is a new massive crisis on top of an already difficult situation,” Save the Children said in a statement.
The outbreak has already had international ripple effects: an American doctor working at Nyakunde Hospital in Ituri has tested positive for the virus. The U.S. Centers for Disease Control and Prevention confirmed that one American has already been evacuated to Germany for treatment, and the agency is working to evacuate at least six other Americans who had close contact with infected patients.
The U.S. government has announced $13 million in emergency humanitarian assistance for the DRC and Uganda, and is considering additional funding through the United Nations’ pooled humanitarian fund, alongside implementing targeted travel restrictions linked to the outbreak. On May 15, after confirmed community spread was documented, the World Health Organization declared the outbreak a Public Health Emergency of International Concern, the highest level of global public health alert.
For now, Congolese authorities say they are drawing on decades of hard-earned experience responding to Ebola outbreaks, relying on tried-and-true public health measures to curb the spread of the 17th Ebola outbreak the country has faced.