The ongoing Ebola outbreak in Central Africa currently centered in the Democratic Republic of the Congo could surge to as many as 20,000 cases or more, a new analysis from U.S. Centers for Disease Control and Prevention (CDC) has warned. The final size of the epidemic will depend entirely on how rapidly response teams can identify and isolate infected people to slow chains of transmission, health officials confirmed Friday.
The CDC released projections from multiple computer-generated scenarios, which forecast a wide range of possible case counts spanning from 10,000 to more than 20,000 total infections. If the worst-case projection holds, the outbreak would come close to matching the deadliest Ebola epidemic in recorded history: the 2014–2016 West Africa outbreak that killed more than 11,000 people and infected over 28,000.
Speaking at a press briefing for reporters, CDC Ebola response incident manager Dr. Satish Pillai emphasized that aggressive public health intervention is the only way to avoid large-scale spread. “Without strong public health interventions, the modeling work suggests an outbreak of that scale is possible,” Pillai said.
Jennifer Nuzzo, director of Brown University’s Pandemic Center, noted that the new projections confirm long-held concerns among infectious disease experts. “This modeling affirms what we have worried about since the beginning: This outbreak is following a dangerous trajectory if more is not done to stop the spread of Ebola,” she said. However, she also cautioned against overreliance on the exact numerical forecasts, noting that outbreak projections are notoriously difficult to get right with limited real-time data. “I wouldn’t read too much into the specific numbers. It’s really hard to make an accurate projection when you have limited data,” Nuzzo added.
As of Friday, the Africa Centres for Disease Control and Prevention has recorded roughly 400 confirmed Ebola cases and 63 confirmed deaths from the current outbreak. Experts widely agree that the actual caseload is higher, as many infections have likely gone undiagnosed and unreported in conflict-impacted regions.
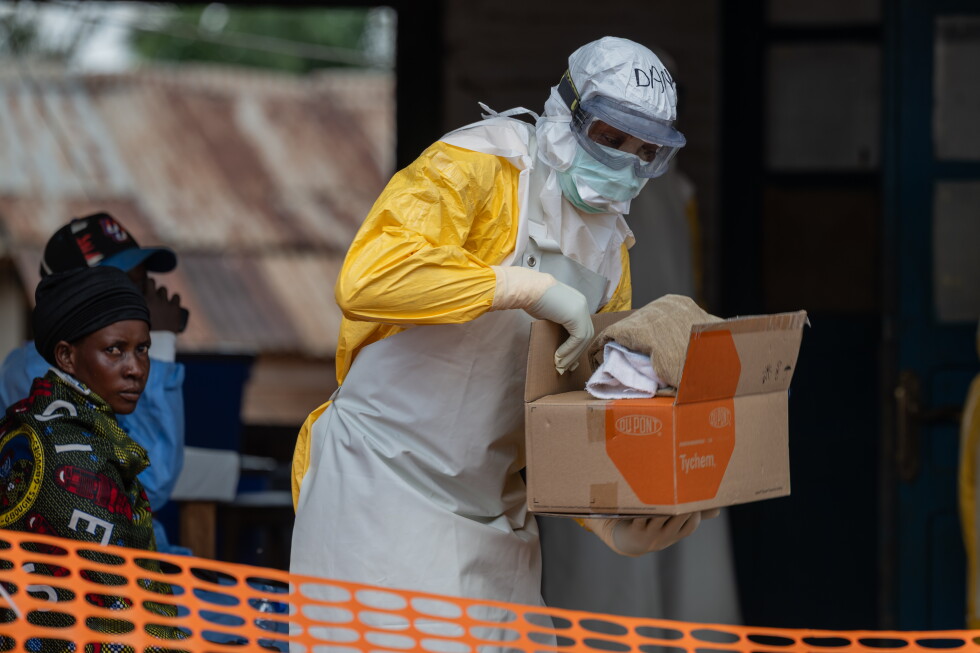
The current outbreak is driven by the Bundibugyo Ebola virus, a strain for which no approved targeted treatments or specific vaccines exist currently. The virus spreads through direct contact with infected bodily fluids including blood, vomit, and semen, and the disease has a high mortality rate. The World Health Organization designated the outbreak a Public Health Emergency of International Concern, the agency’s highest alert level, in May 2024. Retrospective analysis suggests community transmission may have begun as early as February, but initial testing incorrectly targeted a different Ebola strain, delaying a coordinated response.
Response efforts have been severely hampered by ongoing armed instability in eastern DRC. The region is facing active conflict between the Congolese government and Rwanda-backed M23 rebel forces, alongside attacks from the Allied Democratic Force, a group affiliated with the Islamic State. Widespread violence has forced hundreds of thousands of people to flee their homes, disrupting public health outreach and contact tracing efforts.
Despite the alarming projections for the outbreak in Central Africa, both Nuzzo and the CDC have assessed that the risk of large-scale community spread of Ebola in the United States remains very low. “I don’t think it’s a scenario that it’s going to come here and spread broadly,” Nuzzo told reporters earlier this week, a conclusion the CDC echoed in its Friday publication.
The low U.S. risk stems in part from new travel restrictions implemented by the U.S. government: entry is banned for non-U.S. citizens and non-green card holders who have traveled to the DRC, Uganda, or South Sudan in the 21 days prior to their attempted entry. U.S. passport holders returning from those three countries are required to undergo mandatory health screening and enter through one of four designated U.S. airports to monitor for potential symptoms.
The CDC’s latest modeling framework tested a range of variables to generate its projections, including undiagnosed past infections and variation in how quickly response teams can isolate new cases. Under a scenario where roughly 50 people had died by late May and only 20% of infected people were successfully isolated before spreading the virus, most simulations forecast at least 20,000 cases and 4,000 deaths over a three-month period. Pillai noted that the actual current rate of successful isolation is believed to fall on the lower end of the range modeled by the agency.
If response teams can scale up isolation efforts to reach 50% or 70% of infected people quickly, the CDC projects total cases would drop to roughly 10,000. At the same time, officials warned that if the true death toll from late May was higher than currently confirmed, final case counts could end up even higher than the worst current projections.
It is not the first time the CDC has released high-profile Ebola outbreak modeling: during the 2014 West Africa epidemic, the agency projected a worst-case scenario of up to 1.4 million infections if no interventions were implemented, a forecast that ended up being more than 50 times higher than the actual final caseload. That experience has shaped the agency’s current approach to framing projections as possible scenarios rather than definitive predictions, officials noted.
The Associated Press’ health and science coverage receives support from the Howard Hughes Medical Institute’s Department of Science Education and the Robert Wood Johnson Foundation, with the AP retaining full editorial control over all content.